
One size does not fit all: Contextualization for a better COVID-19 response in Northwest Syria
Ola Fahham, Omar Alhiraki
International recommendations for the prevention and control of COVID-19 cannot be extrapolated to all contexts, particularly those affected by protracted conflict. In Syria, the first case of COVID-19 was identified in an area under government control on 23 March 2020, followed by cases in northeast Syria (Autonomous Administration controlled area) in April 2020. It was not until 9 July 2020 that the first case was identified in northwest Syria. Since then, cases have increased rapidly, though accusations that the Syrian government suppressed case reporting in areas under its control persist. Northwest Syria (NWS), an opposition-controlled area in which 4.17 million people shelter (2.7 million of whom are internally-displaced, with around 1.5 million in camps), has been devastated by the rapid escalation of cases. Internationally recommended interventions are either unfeasible, unenforced, or rejected by communities which continue to be bombed. Initial lockdowns were financially devastating for communities, as poverty and unemployment rates are high and many rely on day labour. Many children have known nothing but conflict, and extended school closures, (though potentially effective in limiting transmission), affect not only education but also safty and mental wellbeing. In this blog, we explore the importance of localising recommendations to context by examining COVID-19 in northwest Syria.
Understanding current context
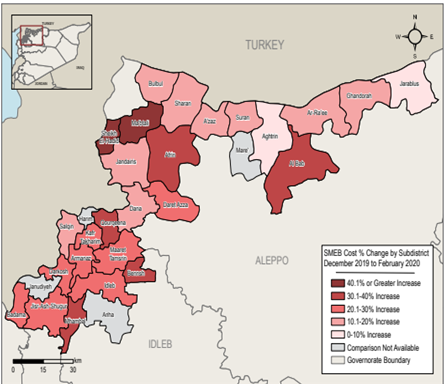
The humanitarian situation in northwest Syria deteriorated significantly since the escalation of military operations by the Syrian government and Russian and Iranian allies in April-August 2019 and December 2019. By March 2020, approximately 1 million people were forced to flee their homes due to escalating violence – most into overcrowded informal camps in northern Idlib and Aleppo governorates with inadequate shelter and WASH (i.e. water, sanitation and hygiene) to meet the basic needs. Ongoing attacks on healthcare, health facility closures and redirection of funds further strained the NWS health system (e.g. 62 health facilities recently closed due to deliberate attacks). Many health-workers have died or been displaced, leaving NWS with only 600 doctors and 64 health facilities – mostly operating as low-capacity field hospitals.
COVID-19 in Northwest Syria
On 9 July 2020, the Early Warning Alert and Response Network (EWARN) confirmed NWS’s first COVID-19 case. Despite the establishment of a COVID-19 preparedness and response plan for Northwest Syria, implementation is fragmented as no single authority can enforce COVID-19 mitigation measures. We identified at least four key actors in Northwest Syria, including the World Health Organization-led COVID-19 Taskforce, the Syrian Interim Government-led COVID-19 National Response Team, de-facto authorities in Idlib, and the Turkish-supported local councils in north Aleppo.
The COVID-19 epidemic increased the burden on NWS’s already overstretched health system. Several factors contribute to increased morbidity and mortality, including:
- high population density, particularly in displacement camps;
- poor health system capacity, particularly for COVID-19 as total numbers of hospital beds, ICU beds, and ventilators are 200, 112 and 83 respectively;
- devastated WASH infrastructure, which includes deliberate interruption and the ongoing violence against health facilities;
- supply constraints, due to the closure of the Bab Al-Salam border crossing with Turkey after the UN Security Council failed to renew the cross-border aid resolution (e.g. the Bab Al-Hawa border crossing is now the only means of importing NWS supplies as the border with government-controlled areas is increasingly impermeable);
- population stress which led to the disregarding of pandemic risks.
Such factors make non-pharmaceutical interventions (NPIs) such as masks, quarantine, physical-distancing, and contact-tracing increasingly unrealistic/underused, particularly in camps, while the socioeconomic effects of attempted mitigation measures negatively affect employment and school attendance.
What context-relevant recommendations can be made?
Prevention is particularly important in northwest Syria, given health system weaknesses, and transmission mitigation measures can be implemented despite challenges. Measures that respect socio-cultural traditions, particularly regarding self-isolation and shielding, are essential to limit transmission. Below we consider masks, WASH, and border restrictions.
Mask-wearing is challenging in Syria due to costs, particularly for disposable masks, as they are not routinely provided free. Nonetheless, masks may be among the most important and simple interventions for use in NWS. Ongoing support and community messaging, including ‘Masks for all’ campaigns, are important as communities have minimal media access. However, it is important that N95 and disposable surgical masks be reserved for health workers who are at the highest risk of nosocomial transmission.
Insufficient WASH services, particularly in camps, limits the value of teaching people to wash regularly – particularly as this is already a strong religious and cultural tradition for many Syrians. What communities usually lack is access to sufficient water quality and quantity and hygiene products. Thus investment in WASH services and resources is urgently needed to enable existing good practices (e.g. many must rely on shared water tanks). Distribution of hygiene kits is similarly insufficient for the existing needs. Cross-cutting community-led WASH improvements are urgently needed.
Although Northwest Syria is an isolated area, with Bab Al-Hawa as the main border crossing, some additional crossings and ‘non-essential travel’ continues. Limited cross-border travel is allowed for supplies, humanitarian workers, doctors, traders, Turkish officials, and military personnel. Limited internal movements continue between northwest, northeast, and government-controlled Syria, though this is predominantly poorly-regulated commercial and smuggling activity. We are critically concerned that if the UNSC does not renew the cross-border resolution in July 2021, northwest Syria will lose its humanitarian aid lifeline for the millions of civilians relying on this support. It is a humanitarian imperative that this border remains open.
The COVID-19 situation in northwest Syria is dire and continues to deteriorate, swamping the already overwhelmed health system and health-workers. Community engagement and community-led initiatives are crucial to identifying effective NPIs to mitigate the continued spread of COVID-19. This is particularly important, as vaccination coverage will unlikely be extensive in Northwest Syria in the near future and is insufficiently effective alone.
Written by Ola Fahham and Omar Alhiraki
Ola Fahham M.D. MPH candidate at University of Nottingham, United Kingdom
Omar Alhiraki M.D. Ex-Trauma and Orthopaedic Resident at Bab Al-Hawa Hospital, Idlib, Syria